
The rapid response required during a stroke care situation is not limited to those who suffer from it outside of hospital walls. Inpatient strokes are as critical as those that happen out of hospital.
Surprisingly, various studies have shed light on the fact that the treatment and evaluation of in-hospital stroke patients often face delays, leading to extended hospitalization and increased disability.
Although protocols exist for treating strokes coming through emergency departments, the same urgency isn’t always present for in-hospital cases.
Research emphasizes the transformative potential of introducing an inpatient code stroke algorithm alongside a targeted educational campaign.
By focusing on bridging the gap between knowledge and timely action, this intervention was successful in improving response times from recognizing symptoms (LSN) to initial assessment and brain imaging.
The findings are particularly significant considering that these response times are directly linked to evidence-supported treatment options for acute stroke care, such as thrombolysis or endovascular thrombectomy.
Such telestroke advancements hold the key to changing the trajectory of inpatient stroke care.
By leveraging telestroke technology, healthcare institutions can offer equitable treatment, whether the stroke occurs inside or outside their walls.
The value of telestroke, in this case, is undeniable, ensuring that every stroke—irrespective of its location—is treated as the emergency it is.
In-hospital strokes, also known as “inpatient” or “hospital-acquired” strokes, can be particularly challenging for several reasons, making these patients at a bigger risk than those whose strokes originate outside of the hospital.
Addressing the unique challenges associated with in-hospital strokes requires increased awareness, staff education, and dedicated protocols to ensure that these patients receive timely and appropriate care.
Telestroke programs can be transformative in addressing the challenges associated with in-hospital strokes.
With immediate access to neurologists specialized in stroke care, even hospitals without on-site neurology expertise can benefit from expert consultations in real-time.
When a patient shows potential symptoms of a stroke, telestroke systems allow for rapid assessment, reducing the chances of misdiagnosing the symptoms as related to another condition or post-surgical effect.
This is particularly crucial since the swift recognition of stroke symptoms can dramatically influence treatment options and outcomes.
Furthermore, telestroke platforms streamline the decision-making process regarding treatments like thrombolysis.
Through remote evaluation using telemedicine technology, specialists can quickly determine the appropriateness of interventions and guide in-hospital teams on best practices and protocols.
This direct line to experts, coupled with the ability to share and review diagnostic images in real-time, helps bypass logistical challenges and minimizes delays, ensuring that in-hospital stroke patients receive care on par with those admitted through emergency departments.
In essence, telestroke programs bridge gaps in care and ensure that in-hospital patients receive timely and evidence-based stroke treatments.
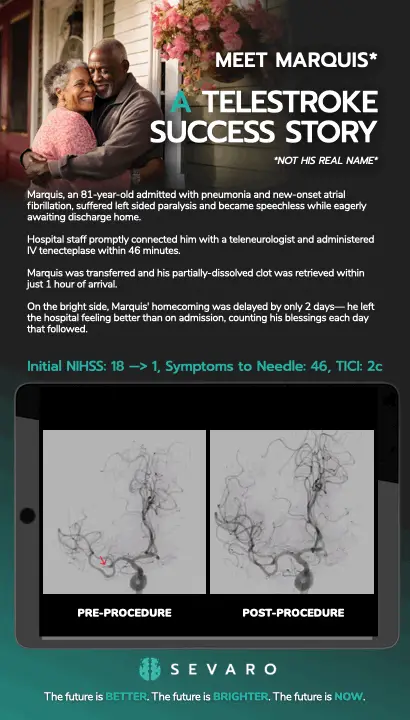
Marquis, an 81-year-old admitted with pneumonia and new-onset atrial fibrillation, suffered left sided paralysis and became speechless while eagerly awaiting discharge home.
Hospital staff promptly connected him with a teleneurologist and administered IV tenecteplase within 46 minutes.
Marquis was transferred and his partially-dissolved clot was retrieved within just 1 hour of arrival.
On the bright side, Marquis’ homecoming was delayed by only 2 days— he left the hospital feeling better than on admission, counting his blessings each day that followed.
Contrary to common logic, stroke treatment and outcomes while hospitalized are less favorable compared to patients outside the hospital. Thankfully for Marquis, well-structured inpatient stroke response and round-the-clock telestroke expertise mitigate inherent disadvantages that admitted patients face.
Early tenecteplase treatment increases the likelihood of stroke recovery, with a 20% clot dissolution rate pre-thrombectomy, triple the odds when combined with thrombectomy, and double the odds of functional independence after three months.
Read more here: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790581
*(subscription required)
In this retrospective study conducted at a Primary Stroke Center, co-authored by Sevaro’s own by Chauncey Evers, the researchers aimed to assess and compare code stroke response times in the Emergency Department (ED) and inpatient settings. Timely stroke care is crucial for positive patient outcomes, and this study sought to provide data for a quality improvement project in the same hospital. The primary objective was to identify areas for improving code stroke response times without compromising the quality of care.
The study analyzed data from 2020, focusing on code stroke care cases that underwent a computed tomography (CT) scan. For cases receiving tissue plasminogen activator (tPA), the researchers examined various time intervals, including code-to-CT scan start, code-to-tPA, CT scan start to tPA, and CT scan completion to tPA. Cases not receiving tPA were also analyzed for response times. The ED’s code stroke response times were compared to those in the inpatient setting.
The results indicated significant differences in response times. In cases receiving tPA, the code-to-CT start time was significantly shorter in the ED compared to the inpatient setting. Similar differences were observed for cases not receiving tPA, including code-to-CT start and code-to-CT read times. The study highlighted a need to improve code-to-CT times in the inpatient setting, as the ED demonstrated more efficient response times.
The findings suggest that addressing the delays in transporting inpatients to the CT scanner after a code stroke activation is essential for improving stroke care quality. The study emphasized the importance of streamlining code stroke responses, implementing standardized protocols, and enhancing interdisciplinary coordination to achieve better outcomes for stroke patients.
Despite some limitations, including a small sample size and the impact of the COVID-19 pandemic, the study’s results underscore the significance of optimizing code stroke response times in both ED and inpatient settings. The proposed changes aim to prioritize early CT scanning, reduce delays, and ultimately save lives while preserving brain function.