
In rural communities, strokes are personal. It’s the grandmother who collapses at a family dinner or the farmer who loses feeling in his arm while working the field. When stroke mortality is higher than the national average and the nearest accredited stroke center is over an hour away, time is of the essence. With the right teleneurology partner, lives are saved and the ROI is unmistakable.
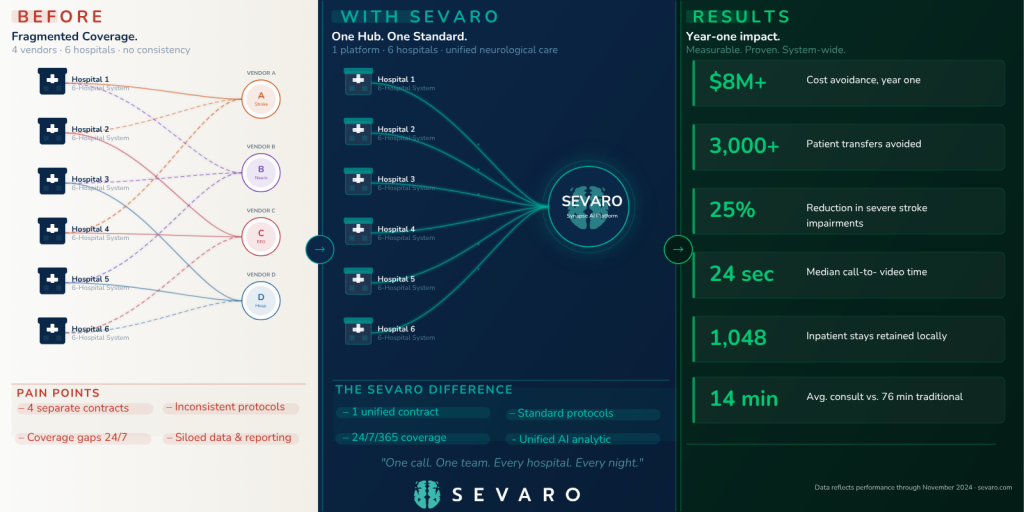
In 2024, a leading health system in rural Tennessee replaced four fragmented teleneurology vendors with a single, unified platform across six hospitals. Within the first year of doing so, the system avoided over 3,000 patient transfers, generated $8M+ by avoiding excess costs, and reduced severe stroke-related impairments by 25%. This is how they got there, and what it means for other systems looking for similar outcomes.
When the health system evaluated its teleneurology infrastructure in 2024, the picture that emerged was inefficient. Four separate vendors were operating across six hospitals, each running its own training programs, escalation workflows, and reporting systems.
There was no shared standard of care or unified data – no way to see how the stroke program was performing as a system. Clinicians adapted and administrators managed the gaps, but the fragmentation was costing the organization in ways that were difficult to see and nearly impossible to quantify.
This was a call to action. For every minute without stroke treatment, nearly two million neurons are lost. In rural Tennessee, those minutes too often become hours. The gap between what patients need and what they can access isn’t simply a system problem. It is a human one, and it is one that a well-built teleneurology program can close.
In May 2024, the health system chose Sevaro, not just as a vendor, but as a partner.
The distinction matters. Sevaro is a physician-founded organization built by neurologists who understand that rural stroke care isn’t a scaled-down version of academic medical centers. It is a fundamentally different challenge that demands purpose-built solutions from people who are genuinely committed to the communities they serve.
Sevaro deployed a unified teleneurology platform across all six facilities, covering both emergent and non-emergent cases from the first stroke alert through ongoing inpatient care. The implementation was built around four pillars, each chosen because they directly impacted what rural hospitals care about most.
The outcomes within the first year set a new benchmark for what rural hospital telestroke ROI looks like when the program is built right.
Within the first year, the health system avoided more than 3,000 patient transfers. 3,000 patients who stayed in their communities, close to the people who know and love them. Telerounding retained 1,048 inpatient stays at local facilities. At an average cost differential of $1,274 per stay, that’s an estimated $8M+ in cost avoidance. But the number that mattered first wasn’t financial.
Severe stroke-related impairments dropped 25%. To understand what that means: in stroke outcomes research, a 2–3% improvement is considered clinically meaningful. A 25% reduction doesn’t just mean the model is working. It means patients are leaving the hospital with more of their lives intact.
Speed reinforced the story. Median consult time hit 24 seconds, with average consults completed in 14 minutes versus 76 minutes under traditional models. These aren’t abstract efficiency metrics, they’re the difference between a patient receiving thrombolytics in time or not. Between a transfer that’s necessary and one that isn’t.
This case is a testament to the power of collaboration, technology-enabled decision-making, and protocol-driven care. It highlights how a well-orchestrated stroke system can dramatically improve patient outcomes by turning a life-threatening event into a story of full recovery.
This partnership was more than operational efficiency. The communities these hospitals serve include some of the most underserved populations in the country, places where, for too long, a patient’s ZIP code determined the quality of their stroke care. That’s not a health system problem. It’s a human one.
By standardizing care across every facility, Sevaro ensured that a patient presenting at a rural hospital received the same caliber of neurological expertise, with the same speed, as a patient at the system’s most well-resourced site. Same evidence. Same protocols. Same standard of care. Every time. Everywhere.
For health systems pursuing stroke certification, Magnet designation, or value-based care arrangements, these equity data carry real strategic weight. For the people living in these communities, it carries something more important: the confidence that their local hospital will be there for them when it matters most.
The experience documented here is a proof point the field has long needed: a rigorous, real-world demonstration that rural hospital teleneurology ROI is not only achievable, but also transformative when the program is built with the right partner and the right structure.
If your hospitals are managing multiple teleneurology vendors, or routinely transferring patients who could be managed locally with the right support, this partnership offers a definitive proof point. Unified teleneurology doesn’t just reduce costs. It keeps patients in their communities, advances health equity in areas where a patient’s ZIP code has too often determined the quality of their stroke care, and builds a program that grows stronger as it scales, compounding returns for the organization and the communities it serves.
For rural hospital leaders evaluating teleneurology ROI, the question is no longer whether a unified teleneurology model delivers measurable returns. This partnership answers that definitively. The question is how quickly your system can move to capture the same results, for your patients, and for the communities counting on you.
Sevaro is a physician-founded virtual neurology company delivering 24/7 telestroke, neurohospitalist rounding, neuro-ICU, EEG interpretation, and ambulatory clinic services, powered by the Synapse AI platform