Stroke 101: What Everyone Needs to Know on World Stroke Day
October 27, 2023
Position title

What Is World Stroke Day?
World Stroke Day is an annual event observed on October 29th, which aims to raise awareness about stroke and its global impact. World Stroke Day is an annual event observed on October 29th, which aims to raise awareness about stroke and its global impact.
Organized by the World Stroke Organization (WSO), this day focuses on educating the public on the signs and symptoms of a stroke, the importance of immediate medical attention, and the long-term care and support that stroke survivors may need. The event also emphasizes the prevention strategies individuals can adopt to reduce their risk of a stroke.
This article seeks to demystify the basics of a stroke, recognizing early signs, preventing strokes through healthy lifestyle choices, and the science behind it, ensuring that you walk away with a clear understanding.
Understanding the Basics of a Stroke
What is a Stroke?
A stroke is a sudden interruption in the blood supply to the brain. Whether because of a blockage or bleeding, it’s a medical emergency that requires immediate attention. With millions affected by it globally, strokes are a leading cause of death and disability.
Why Do Strokes Happen?
At its core, a stroke is about the brain not getting the nutrients and oxygen it needs to function, typically due to blocked or ruptured blood vessels. Without the vital flow of blood, brain cells start to die, leading to potential long-term damage or death.
Different Types of Strokes
Ischemic Stroke
This type of stroke occurs when there’s a blockage in a blood vessel supplying blood to the brain. It’s the most common kind, accounting for about 80% of all strokes. These blockages are typically caused by blood clots or the buildup of fatty deposits and other debris.
Hemorrhagic Stroke
Hemorrhagic strokes are caused by bleeding within or around the brain. This can result from conditions like aneurysms, which are weakened, bulging sections of blood vessel walls, or arteriovenous malformations (AVMs), tangles of malformed blood vessels.
Transient Ischemic Attack (TIA)
Often referred to as a “mini-stroke”, a TIA resembles an ischemic stroke but doesn’t last as long and doesn’t cause permanent damage. Even though the effects of a TIA are temporary, it’s crucial to seek medical attention as it could be a warning sign of a future stroke.
The Science Behind a Stroke
Brain Cells and Their Need for Oxygen
Each of our brain cells needs a steady supply of oxygen to function. This oxygen is delivered via the blood. When there’s an interruption, brain cells become deprived and begin to die, which can lead to lasting damage or even death.
How Blood Flow Gets Interrupted
Picture a smoothly flowing river, and now imagine a dam suddenly blocking it. That’s what happens during an ischemic stroke. On the other hand, imagine the riverbank suddenly bursting, causing flooding—that’s akin to a hemorrhagic stroke.
Recognizing the Signs of a Stroke
The BEFAST Method:
When suspecting someone might be having a stroke, remember the acronym BEFAST:
- B (Balance): Sudden loss of balance or coordination.
- E (Eyes): Sudden trouble seeing out of one or both eyes or double vision.
- F (Face): Ask the person to smile and check if one side of the face droops.
- A (Arms): Ask the person to raise both arms and see if one arm drifts downward.
- S (Speech): Ask the person to repeat a simple phrase and listen for slurred or strange speech.
- T (Time): If you notice any of these signs, it’s time to call 911 or emergency services immediately.

Other Potential Stroke Warning Signs
Keep an eye out for sudden numbness or weakness, especially on one side of the body, sudden confusion, trouble seeing in one or both eyes, trouble walking, dizziness, or an unexplained severe headache.
The Importance of Immediate Action For Stroke
Time is Brain
In stroke treatment, every second counts. The earlier a person gets treatment, the better their outcome is likely to be. In fact, getting to a hospital within 4.5 hours of the first symptoms can greatly reduce the risk of long-term disability.
Seek Immediate Medical Attention For Strokes
When you or someone else displays signs of a stroke, it’s essential to call emergency services right away. Also, remember to note when the symptoms first began, as this can influence treatment decisions.

Stroke Prevention: Lifestyle Choices That Make a Difference
What are the biggest Stroke Risk Factors?
- High blood pressure: Often termed the “silent killer,” it’s the leading cause of stroke.
- Diabetes: High sugar levels can lead to clotting more easily.
- High cholesterol: Fatty deposits can clog your blood vessels.
- Smoking: Nicotine raises your blood pressure.
- Alcohol consumption: Excessive drinking can lead to multiple health complications, including stroke.
- Family history: Stroke can sometimes run in the family.
The Power of a Balanced Diet
Eating a balanced diet is vital for overall health and particularly beneficial for stroke prevention.
- Incorporate whole grains, fruits, and vegetables: These provide essential nutrients and antioxidants.
- Limit saturated fats and sugars: Helps maintain a healthy weight and reduces cholesterol.
- Importance of hydration: Drinking water aids in maintaining blood volume and viscosity.
Embracing Regular Exercise
Physical activity has numerous health benefits, one of which is stroke prevention.
- Aerobic activities: Walking, cycling, or swimming can improve heart health and reduce stroke risk.
- Strength training and flexibility exercises: Builds muscle and maintains joint health.
- The connection between physical activity and reduced stroke risk: Active individuals generally have lower cholesterol and healthier blood pressure levels.
The Importance of Smoking Cessation
Smoking accelerates clot formation by thickening your blood and increasing the amount of plaque buildup in arteries.
- How smoking increases stroke risk: Nicotine and carbon monoxide from inhaling smoke reduce the amount of oxygen your blood can carry.
- Benefits of quitting smoking: Enhanced lung capacity, reduced blood pressure, and improved blood circulation within a few weeks.
Regular Health Check-ups: Prevention is Better than Cure
It’s essential to keep an eye on potential risk factors.
- Monitoring blood pressure: Consistent high readings are a significant red flag.
- Regular cholesterol checks: Ensures you maintain a healthy balance of lipids.
- Diabetes management: Monitoring sugar levels to prevent complications.
The Digital Revolution: How Technology is Transforming Stroke Care with telestroke
The Pivotal Role of Technology in Stroke Care
Historically, diagnosing and treating strokes depended heavily on a patient’s symptoms and basic imaging. Now, we harness technology to offer more precision, speed, and efficiency.
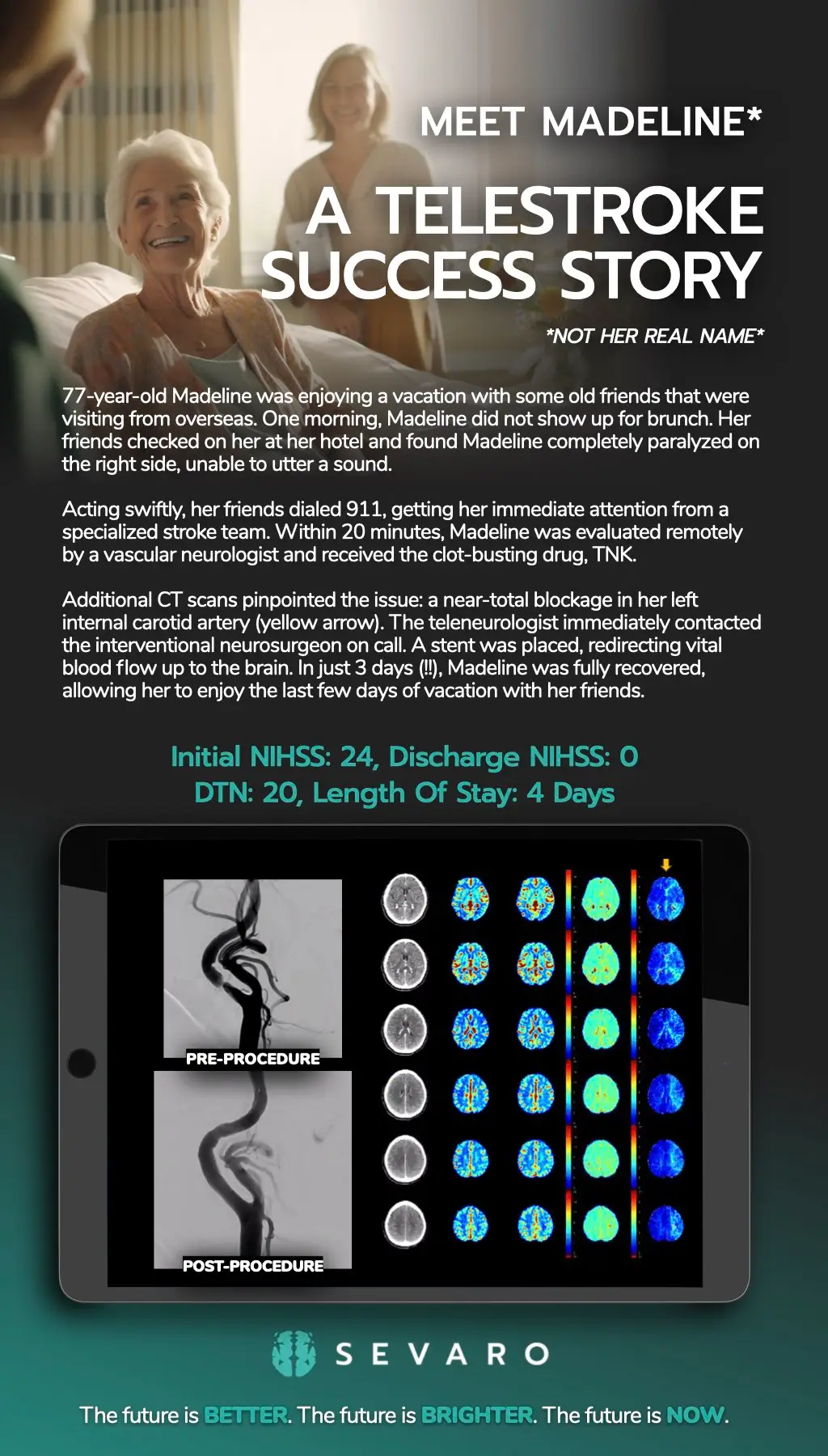
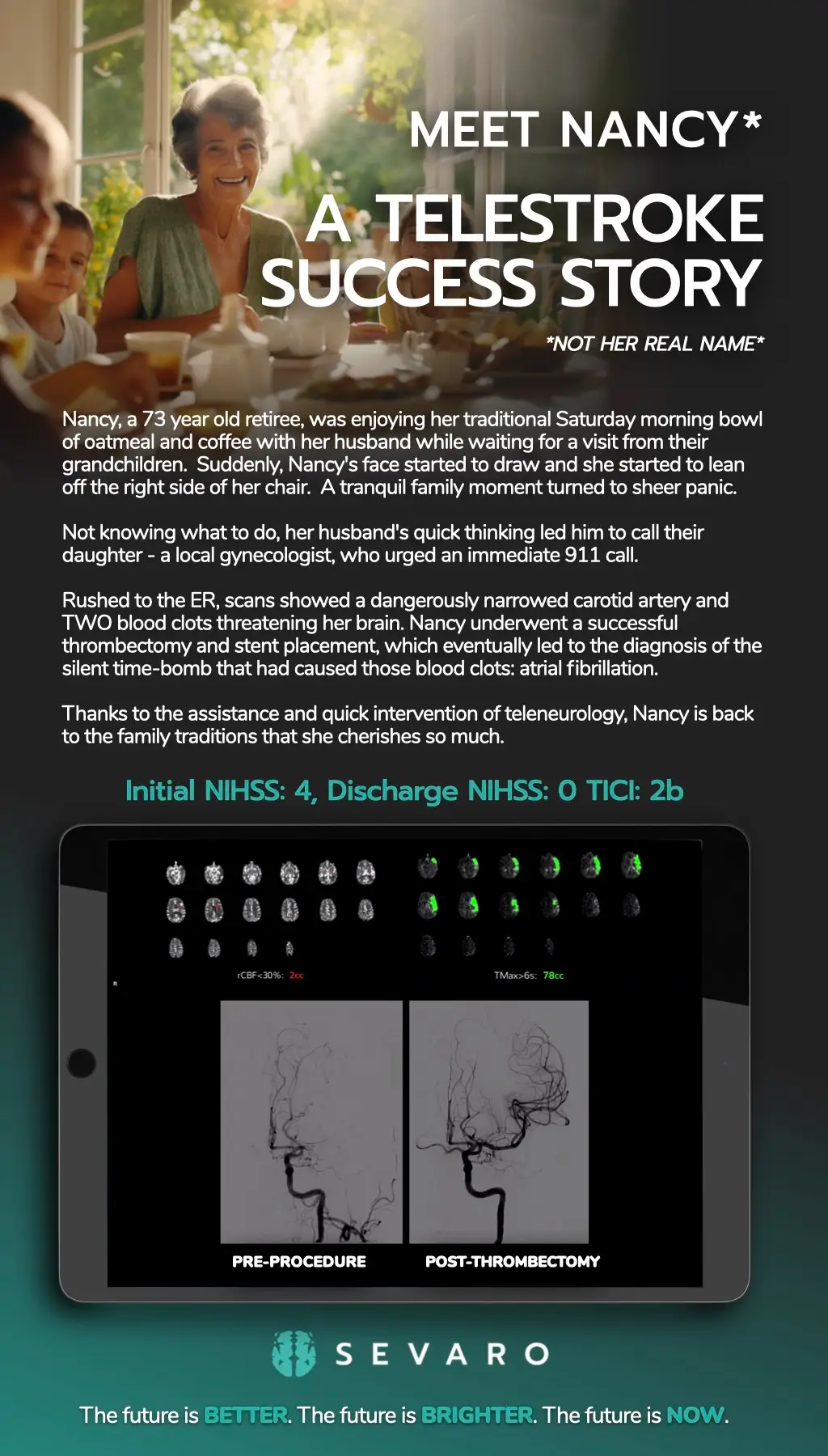
What is Telestroke?
Telestroke is a telemedicine approach that facilitates the consultation of stroke specialists for patients in remote or underserved areas using digital communication.
Benefits of Telestroke Services
- Immediate access to specialists: Reduces the ‘door-to-needle’ time.
- Reducing time-to-treatment: Prompt treatment can mean the difference between recovery and long-term disability.
- Improved outcomes for patients: Access to specialists leads to better patient care and outcomes.
Revolutionizing Stroke Diagnosis
- Speed of detection: AI can quickly analyze data and detect abnormalities.
- Precision and accuracy: Fewer human errors mean better patient outcomes.
- Data analysis for more informed decisions: AI algorithms can analyze vast amounts of data rapidly, providing more informed treatment recommendations.
The Stroke Recovery Process: A Journey of Healing and Hope
Experiencing a stroke is undoubtedly a significant and life-altering event, but the journey doesn’t end once the immediate threat has passed. The road to recovery post-stroke is often long and requires patience, determination, and a multidisciplinary approach. Here’s a closer look at the stroke recovery process, giving hope and guidance to patients and their families.
1. Understanding the Phases of Recovery
- Immediate Phase: This usually lasts for a few days post-stroke and focuses on stabilizing the patient, preventing complications, and beginning early rehabilitation.
- Rehabilitation Phase: This phase can begin as early as 24 hours after a stroke and can last for several months or even years. It’s a period of structured recovery with the help of medical professionals.
2. The Role of Rehabilitation
Rehabilitation aims to help patients regain their lost abilities and learn to cope with any residual disability.
- Physical Therapy: Helps restore physical functions such as walking, balance, and coordination.
- Occupational Therapy: Aims to help patients regain daily living skills like eating, dressing, and bathing.
- Speech Therapy: Assists patients in relearning language and communication skills. It also addresses swallowing difficulties.
- Neuropsychological Therapy: Addresses cognitive deficits such as memory problems, attention deficits, and other related issues.
3. The Importance of a Support System
Recovery is not just a physical journey; it’s an emotional one too.
- Emotional Support: Many patients experience feelings of frustration, depression, or anxiety post-stroke. Having a robust support system – including family, friends, and support groups – can be invaluable.
- Educational Resources: Understanding the recovery process can ease feelings of uncertainty. Seek out resources, attend workshops, or join support groups.
4. Setting and Celebrating Milestones
Every individual’s recovery journey is unique. While some might regain abilities quickly, others may find progress slower.
- Goal Setting: Work with your rehabilitation team to set short-term and long-term goals. Celebrate every milestone, no matter how small.
- Patience and Persistence: Recovery can be a slow process, but every step forward is a victory.
5. Adapting to a New Normal
Post-stroke, patients may have to adapt to a ‘new normal’, embracing certain lifestyle changes and modifications.
- Home Modifications: Simple changes like installing grab bars, using a shower chair, or rearranging furniture can make daily living easier.
- Lifestyle Choices: Embracing a heart-healthy diet, engaging in regular exercise (as advised by the therapist), and avoiding smoking or excessive alcohol can prevent recurrent strokes.
My Stroke Journey: Sevaro’s Support For Stroke Survivors
Sevaro presents “My Stroke Journey,” a free monthly support group dedicated to assisting stroke survivors and their caregivers. Recognizing the profound life changes that accompany a stroke for both patients and their families, Sevaro aims to provide ongoing support well after hospital discharge.
With a team comprising neurologists, therapists, educators, and mental health professionals, these virtual sessions address the emotional and physical ramifications of strokes and offer coping strategies.
Guided by Stroke Ambassador Pete Smith, a stroke survivor himself, the sessions inspire and guide attendees to find resilience and hope in their post-stroke life.
In Summary
Strokes remain a formidable global health concern, affecting millions each year and serving as a major cause of death and long-term disability. This article endeavored to enlighten readers about the basics of strokes, from understanding their genesis, the distinct types, and the science that underpins them.
Recognizing early signs of a stroke, epitomized by the BEFAST method, could mean the difference between life and death. Prompt action, paired with the understanding that “Time is Brain,” maximizes recovery chances.
But knowledge doesn’t stop at recognition and rapid response. Embracing positive lifestyle habits – like a nutritious diet, regular exercise, smoking cessation, and routine health check-ups – can play a pivotal role in stroke prevention. As we look to the future, technological advancements, such as telestroke services and AI diagnostics, are revolutionizing stroke care, offering increased accuracy, swiftness, and accessibility.
On World Stroke Day, and every day, awareness and education remain paramount. With the knowledge you’ve gained from this article, you’re better equipped to not only protect yourself but also to serve as an advocate for stroke awareness in your community. Together, we can make strides in the fight against this pervasive medical emergency.