118 Minutes to 40: How Sevaro's Teleneurology Partnership Made St. Mary's a National
Leader in Stroke Care
“Before our partnership, St. Mary’s time to treat a stroke patient from arrival was 118 minutes. Thanks to Sevaro, it’s been reduced to just 40 minutes, and continues to improve.”
Industry Background
Every year, 800,000 Americans experience a stroke. Stroke is the leading cause of disability in the United States; in addition to weakness and numbness, stroke can also lead to changes in cognitive function and memory.
Clot busting medications, called thrombolytics, can treat stroke patients and reverse the symptoms if presented to medical attention quickly enough. Thrombolytics are approved to be given within 4.5 hours of stroke symptoms starting. The data shows that the sooner you give this medication, the better it works in reducing or eliminating stroke symptoms. Door-to-needle time refers to the time from when a patient presents to hospital to the time the medication can be given.

The Partnership
Sevaro is a teleneurology company with a team of subspecialty trained vascular neurologists who have a passion for delivering the most up-to-date stroke care with the latest medical technology. Sevaro partnered with St. Mary’s Hospital in Q4 of 2019. The two teams collaborated, reviewing the current state and process of stroke care, and identified areas for improvement. Namely, how could Sevaro help St. Mary’s provide more efficient stroke care resulting in better patient outcomes and improved health care utilization?
The Sevaro team identified areas for improvement including time to CT, door-to-needle times, increased utilization of stroke order admission set, and decreased length of stay. In order to continuously improve, the data from each stroke case was carefully collected and reviewed. St. Mary’s went live with Sevaro in November, 2019.
The Result
- From 2020 to 2021 the time from patient arrival to neurology notification has improved by over 3 minutes.
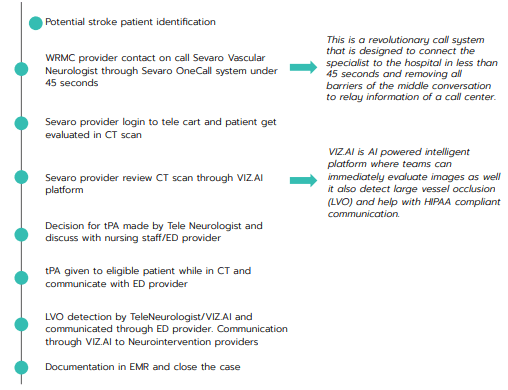
- Call centers have been removed, and now ED teams connect directly with stroke neurologists within 45 seconds.
- Total of 315 stroke code activated in 2021
- 83% increase in tPA use (1/month in 2019 to 22 in 2020)
- Zero missed eligible patients offered thrombolytics since implementation
- Decreased door to needle time! Time from patient presentation to treatment reduced from 118 minutes to a 40 minute average in 2022 (with a best time of 20 minutes in 2021).
- Improvement in stroke patient order sets utilization during admission to St. Mary’s resulting in more patients being treated and managed with guidelines directed therapies
- Zero patients discharged without appropriate cholesterol management.
- Named a 2021 Silver Plus with Honor Roll member from the American Heart Association and American Stroke Association.
- Implemented artificial intelligence software to assist clinicians in identifying strokes on brain imaging
Summary
After partnering with Sevaro, St. Mary’s is able to provide expert neurologic consultation within 45 seconds for patients presenting with stroke symptoms. Sevaro’s fast, easy-to-use platform allows for reduction in door to treatment times, increased use of stroke-directed therapies, and improved access to specialized neurologic care.
Once patients are admitted to St. Mary’s, the quality improvement efforts have continued. Now, more patients are treated under the stroke order set; this implementation translates to more patients being discharged on the guideline recommended medications and reducing their length of stay in the hospital. This all culminates in improved patient outcomes, and positions St. Mary’s to be a national leader in providing exceptional stroke care.